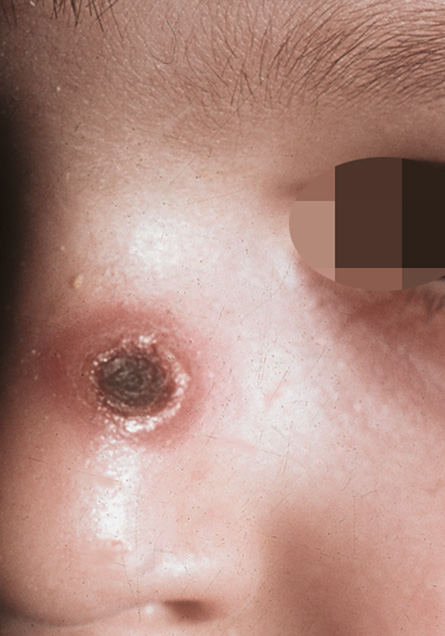
Necrotizing granulomatous folliculitis of the nose.
Downloads
DOI:
https://doi.org/10.26326/2281-9649.29.2.1992How to Cite
Abstract
These two cases share the history – inflammatory lesions arisen in the summer on the nose, the first necrotizing with eventual depressed scarring and the subsequent ones non-ulcerated, all asymptomatic and spontaneously regressing after 3-12 months –. Both children were in good health, they were immunocompetent, they had no history of infectious diseases, they did not suffer from acne or other lesions of the face and had been not affected by chalazia. Clinical and histological data allowed us to exclude leishmaniasis, herpetic infections (4), acne (2), rosacea, idiopathic facial aseptic granuloma, granuloma faciale and chronic granulomatous disease. Arthropod stings can be responsible for granulomatous and necrotizing folliculitis. Lee et al. (3) described granulomatous folliculitis after apitherapy (bee sting or injections of bee venom extracts) in vogue in Asia for neuralgia and arthralgia. Ruiz- Maldonado et Al. (5) described severe hypersensitivity reactions to arthropods with hydroa vacciniforme type scarring in photoexposed sites in children; such reactions are sometimes the expression of lymphomas. We know that in reactions due to hypersensitivity to mosquito the first reactions can be bullous, whereas the following ones are classic papular-pomphoid lesions (1): this could explain the greater intensity up to the cicatricial necrosis in the first lesion in both cases.